
Breathing – Part I – Anatomy & Mechanics
呼吸-Part I-解剖學&機制
The average person takes about 21,000 breaths a day. This makes it one of the 3 biggest aspects of our patients life that we can have a profound effect on (other 2: posture & walking).
人們平均每天會進行21000次的呼吸,這使得呼吸變成是我們可以對病人生命有著深遠影響的三個最大面向的其中一個(另外兩個是:姿勢&行走)
This post will discuss the holistic effects of breathing, anatomy, and the important cascade of events for proper breathing and inner core stabilization.
本篇文章將會討論呼吸的整體效果、解剖構造(學),以及對適當呼吸與內部核心穩定性而言重要的級聯事件Why Work On Breathing? 為何要致力於呼吸?
Because everyone is doing it. Power lifters have been controlling their intra-abdominal pressure to lift massive weights for years. Yoga and eastern medicine have been using breathing for over 2,000 years (PT isn’t even a century old) .
因為每個人都要呼吸。健力選手已經控制他們的腹內壓來舉起巨大重量好幾年了;瑜珈與東方醫學已經使用呼吸超過2000年了。(物理治療甚至還沒滿一世紀)
Gray Cook and the SFMA require a full breath at the end-range of every movement test to achieve a FN. The neuro-orthopedic approach leans on breathing and even mentions that a deep breath glides the median nerve 1 inch.
Gray Cook與SFMA要求在每一個動作測試的末端範圍能有著完整的呼吸來達到FN(功能性、無疼痛)神經骨科手法/方法倚靠在呼吸上且甚至提到"深呼吸能使正中神經滑動1英吋"
There is an increasing amount of approaches that are including breathing (PRI, SFMA, DNS). Many of the leading experts in the field are incorporating breathing. And there is more and more research coming out discussing the benefits of breathing. So if you’re not doing it, or at least aware of it, then you are probably that guy.
將呼吸列入其中的流派越來越多(PRI、SFMA、DNS)
領域中許多權威專家都併入了呼吸,也有著越來越多討論呼吸益處的研究出爐
所以如果我們不去做,或至少意識到它,我們可能就是"那個人"
Holistic Breathing 全面/整體的呼吸
Breathing has a huge influence on the entire body. Breathing influences sympatho-vagal balance. Dyfunctional breathing can induce hypocapnia (effect of hyperventilation).
呼吸對整個身體有著巨大的影響,呼吸會影響交感-迷走神經平衡功能障礙的呼吸可能引起低碳酸血症(過度換氣的結果)
Hypocapnia causes increased neural activity and synaptic transmission. You know those patients that feel that every muscle is tight and you can never decrease their muscle tone for more than 24 hours?
低碳酸血症導致升高的神經活動與突觸傳遞,你認識那些感覺每一條肌肉都是緊繃且我們永遠無法減低他們的肌肉張力多過24小時的病人嗎?
Maybe it’s because of their breathing. Breathing can actually produce an amplification of the parasympathetic nervous system. This can have a tremendous effect on muscle tone (a nervous system issue).
或許那是因為他們的呼吸,呼吸實際上可以引起副交感神經系統的增幅,而這對肌肉張力能有著巨大影響(神經系統的問題)
Breathing also has a significant role in the circulatory system, pH regulation, and metabolism. It has been tied to many psychological disorders and can have a major effect on self-regulation of stress and emotion. Breathing even has an important role in some religions and spiritual practices.
呼吸在循環系統、pH調節與代謝中也有著舉足輕重的地位(重要影響)呼吸已經被與許多心理失調相關聯,且對壓力與情緒的自我調節有著重大影響
呼吸甚至在某些宗教與精神修行中扮演著重要腳色
Breathing has a therapeutic, homeostatic, regulatory, psychophysiological, and spiritual function. If your patients are alive, then breathing should be considered as an aspect of their care.
呼吸有著治療性、體內平衡、調節性、心理生理與精神的功能,如果你的病人是活著的,那麼呼吸就應該要被視為是他們需要操心的一個面向Breathing Anatomy 呼吸解剖結構
A global understanding of breathing anatomy can be expanded from knowledge of the deep front line. This line from Anatomy Trains goes into the fascial attachments of the diaphragm in great detail. Or simply stated, “the 12th rib is where walking meets breathing“-Tom Myers.
一個呼吸解剖結構的全面性認識可以從"深前線"的知識來擴展,這條來自解剖列車的線十分充分徹底的進入橫膈膜的附著處,或者我們簡單的說"第12肋骨是步行遇到呼吸之處"-Tom Myers.Diaphragm 橫膈膜
The diaphragm has a dual function: respiration and stability. It should be able to perform this dual function at all times. A common injury is caused by a failure of this mechanism.
橫膈膜具有雙重功能:呼吸作用與穩定度,它應該要能在所有時候執行這種雙重功能,常見的傷害是由此種機制的失效所導致
The overweight, sedentary, desk-jockey wakes up to shovel snow out of his driveway. After 5 minutes he’s exhausted and his diaphragm has to devote all of its power for respiration. Now his diaphragm has lost it’s stability function. Now he can’t control and use his intra-abdominal pressure (IAP). And now he just hurt his back.
一位過重、久坐的辦公桌人早上醒來去將雪鏟離車道,在五分鐘後他筋疲力盡、他的橫膈膜把所有的精力都投注在呼吸作用。現在他的橫膈膜已經失去了穩定的功能,現在他無法控制與使用他的腹內壓(IAP)
然後現在他傷到他的背部了
Want another reason why we should know about the diaphragm’s stability role? It’s the most proximal muscle…to everything. There’s nothing more proximal than the diaphragm. It helps to organize and stabilize the upper and lower quarter. Sue Falsone agrees that the diaphragm is the most proximal. Regarding this concept she has said that she always starts rehab “from the belly button out.”
想要其他為什麼我們應該要認識橫膈膜的穩定度腳色/任務/作用的原因嗎?橫膈膜是最近端(近身體中心)的肌肉...對所有事物來說,沒有什麼比橫膈膜更加靠近身體中心
橫膈膜能幫助組織與穩定上下半身,Sue Falsone同意橫膈膜是最近身體中心的,而關於這個概念,她曾說她總是從肚臍開始向外修復/復健
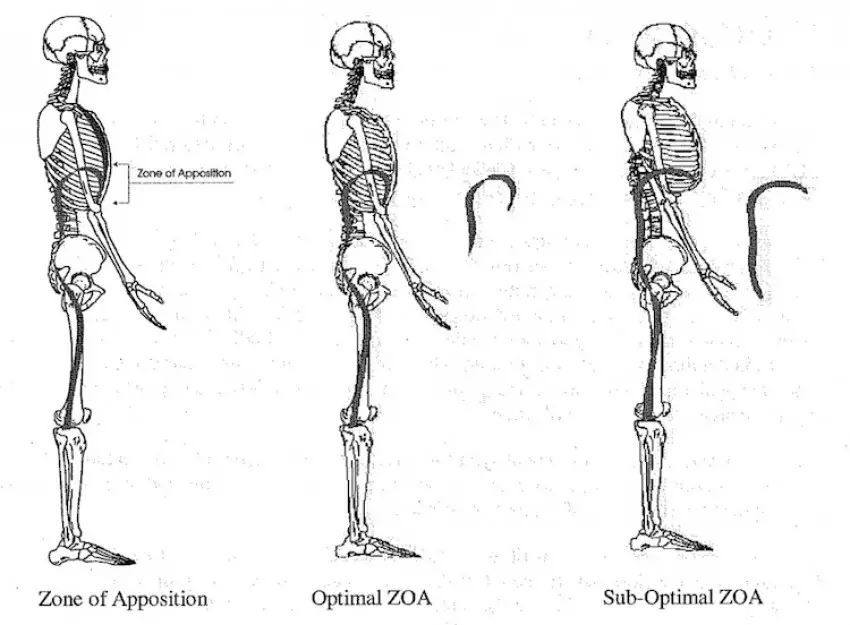
Zone of Apposition 並列區域
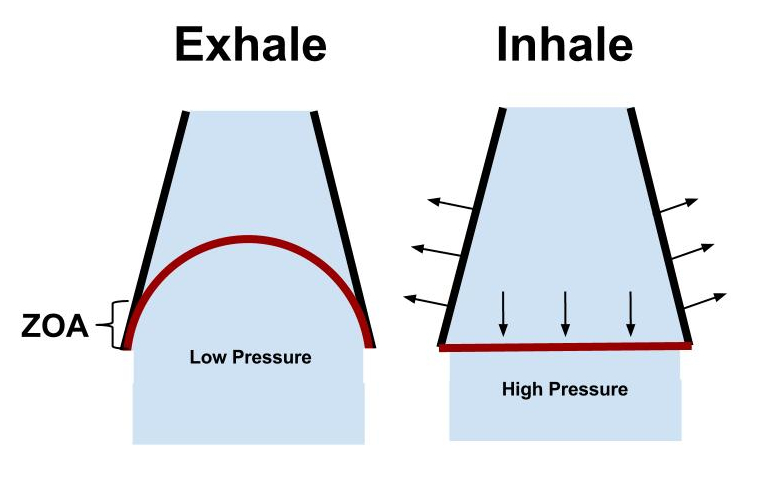
The Postural Restoration Institue defines the ZOA as the “cylindrical aspect of the diaphragm that apposes the inner aspect of the lower mediastinal (chest) wall.” This is one of the most important aspects of breathing.
Postural Restoration Institue將ZOA定義為"與下段胸廓內面並列的橫膈膜圓柱面",這是其中一個呼吸最重要的面ZOA(並列區域)主要的責任是:
- Efficient length-tension relationships of the diaphragm
高效的橫膈膜長度-張力關係 - Maintains vertical alignment of diaphragm muscle fibers
維持橫隔膜肌肉纖維的垂直排列 - Allows postero-lateral (bucket-handle) movement of the lower rib cage
讓下段胸廓得以有著後-側向的動作(水桶提把)
Overall the ZOA is paramount for proper diaphragm function. Some have found it to be as much as 30% of the inner surface of the ribcage.
總地說來,對適當的橫膈膜功能而言ZOA是最重要的,有些人發現ZOA幾乎多達胸廓內部表面的30%
A decreased ZOA will result in inefficient diaphragm contraction, lung hyperinflation, increased accessory muscle use, lack of postero-lateral movement of the rib cage, and an increased anterior rib flare.
縮小的ZOA將導致無效率的橫膈膜收縮、肺部充氣過度、升高的附屬肌肉使用、缺乏後-側向的胸廓動作,以及增加的前側肋骨外翻(Rib flare)
Postural Restoration Institute (PRI) – Zone of Apposiion (www.posturalrestoration.com)
Abdominals & Pelvic Floor 腹部肌群&骨盆底肌
The abdominals and pelvic floor play a huge role in inspiration (eccentrically) and expiration (concentrically). During inspiration they contract eccentrically to increase the intra-abdominal pressure (i.e. stability) and ensure that the ZOA is maintained long enough to produce postero-lateral expansion of the lower ribcage. During expiration they concentrically contract to help push the diaphragm cephallically, thus restoring optimal ZOA.
腹部肌群與骨盆底肌在吸氣(離心)與吐氣(向心)中扮演著重要角色在吸氣過程中它們離心的收縮來增加腹內壓(穩定度)並確保ZOA被維持在足以引起下段胸廓後-側向的擴張之長度
在吐氣過程中它們向心的收縮來幫助往頭頂方向推動橫膈膜,從而恢復最佳的ZOA
Thoracic Cavity 胸腔
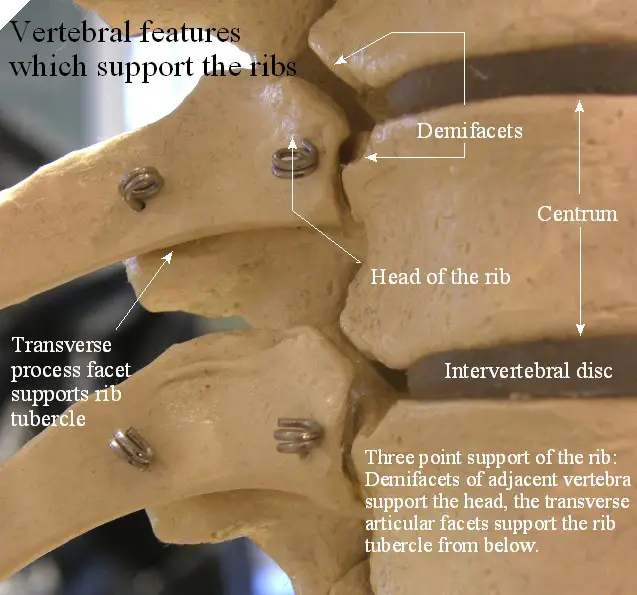
Ribs act as a lever to elongate the thoracic spine 肋骨向槓桿般動作來拉長胸椎
The thoracic cavity is where the actual breath occurs. It’s where the air molecules and gas exchange occurs. The thoracic cavity must have the appropriate amount of mobility to accommodate this pressure change and flow of molecules. During inspiration the ribs must be able to ER and the spine must be able to extend. During expiration the ribs must be able to IR and the spine must be able to flex.
胸腔是呼吸真正發生的地方,它是空氣分子與氣體交換發生的位置胸腔必須要有著合適之活動度的量來容納這種壓力改變與分子流動
在吸氣過程中,肋骨必須要能夠外旋(ER)、脊椎必須要能夠伸展
在吐氣過程中,肋骨必須要能夠內旋(IR)、脊椎必須要能夠屈曲
Breathing plays a major role in the hydration of the thoracic discs. If you look at the anatomy of the ribs attachment to the thoracic spine it almost looks like a lever. This lever actually pry’s open the thoracic spine and elongates it, thus bringing hydration and nutrition to the discs.
呼吸在胸椎椎間盤的水合作用中起著重要作用,如果我們去看肋骨與胸椎連接處的解剖構造,那看起來就像個槓桿,而這個槓桿實際上會撬動胸椎並拉長它,從而將水合作用與營養帶到椎間盤
Breathing Mechanics (Core from the Inside Out)
呼吸機制(由內到外的核心)
There is a cascade of events that leads to controlled intra-abdominal pressure through the activation of the diaphragm and core musculature.
有個導致有控制的腹內壓(透過橫膈膜與核心肌群的活化)之級聯事件
By using the breath with the core you are achieving natural muscle activation and increased intra-abdominal pressure. This pressurized stability is much more efficient than muscle activation alone (abdominal hallowing/isolated TVA activation).
透過結合核心使用呼吸我們正在達成自然的肌肉活化與增加的腹內壓這種加壓的穩定度比單獨的肌肉活化更加有效率(腹部挖空/孤立的腹橫肌活化)
The best way to have a proper breathing pattern is to get it right from the inhale. A proper inhale will put you in the correct position for a proper exhale. Clinically there are many things that can go wrong with inspiration, whereas the only thing that often goes wrong with expiration is decreased expired air (hyperventilation/decreased ZOA).
有著恰當呼吸模式的最佳方式是從"吸氣"開始搞對恰當的吸氣會將我們擺在一個正確的位置以恰當的吐氣
臨床上吸氣有很多事情可能會出錯,但吐氣經常出錯的唯一一件事是呼出氣體的縮減(過度換氣/縮小的ZOA)
The inhale is the initiation of core stability.
吸氣是核心穩定度的開始。Inspiratory Cascade of Events 吸氣級聯事件
1) Diaphragm Concentrically Contracts
橫膈膜向心性收縮
Having a proper ZOA allows for an efficient start of inspiration
有著恰當的ZOA讓我們可以有著吸氣的高效起始點
有著恰當的ZOA讓我們可以有著吸氣的高效起始點
2) Beginning of Increased IAP
升高的腹內壓之開始
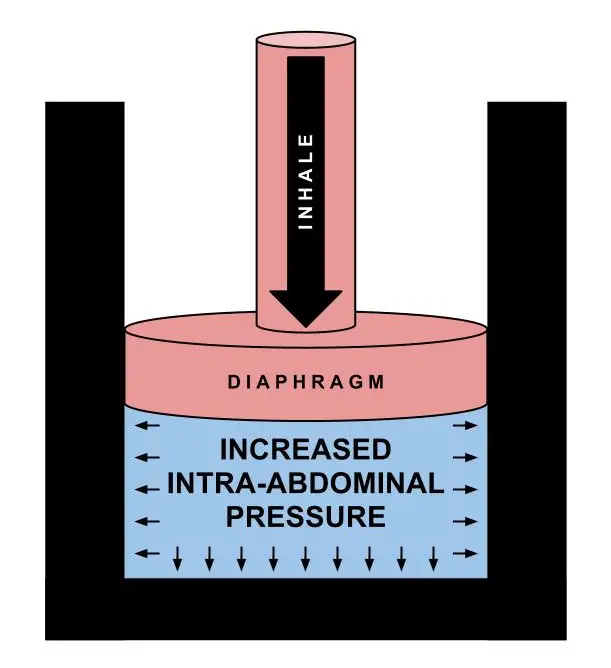
Contraction of the diaphragm acts as a pistol, creating increased IAP
橫膈膜的收縮像是手槍(活塞?),造成升高的腹內壓
橫膈膜的收縮像是手槍(活塞?),造成升高的腹內壓
3) Abdominals and PF Eccentrically Contract
腹部肌群與骨盆底肌離心性的收縮
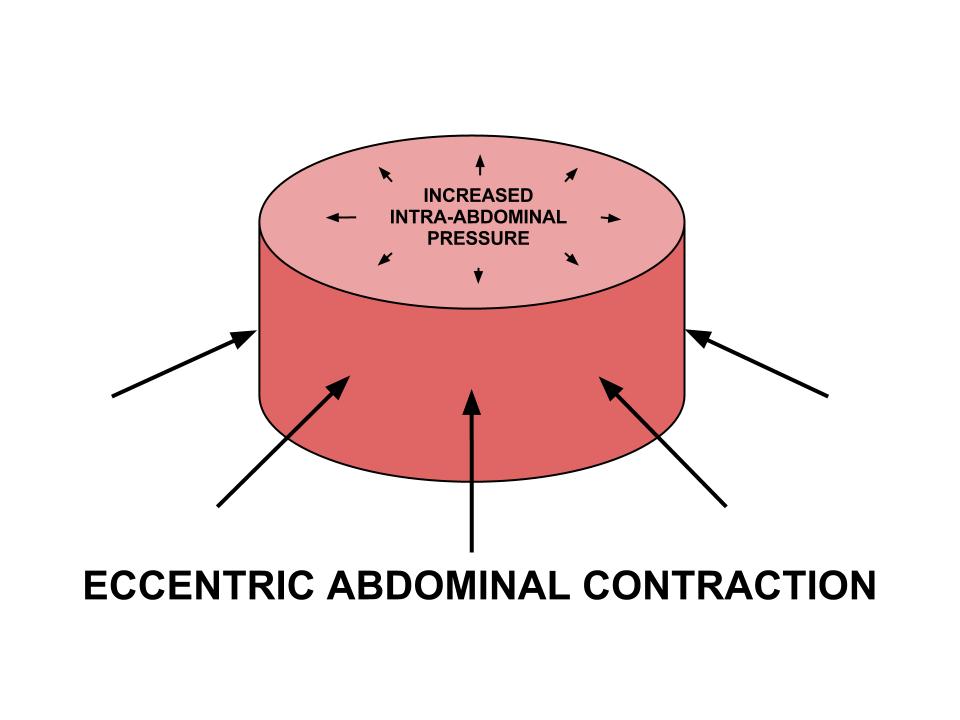
Increased IAP is optimized with an eccentric contraction of the abdominals & PF. This maintains ZOA and causes 3-dimensional expansion of the lower ribcage.
結合腹部肌群與骨盆底肌的離心收縮能使增加的腹內壓最佳化
這樣能維持ZOA並導致下段胸廓的3D擴張
結合腹部肌群與骨盆底肌的離心收縮能使增加的腹內壓最佳化
這樣能維持ZOA並導致下段胸廓的3D擴張
4) Controlled Increase in IAP & Inner Core Stability
腹內壓與內部核心穩定度有控制的增加
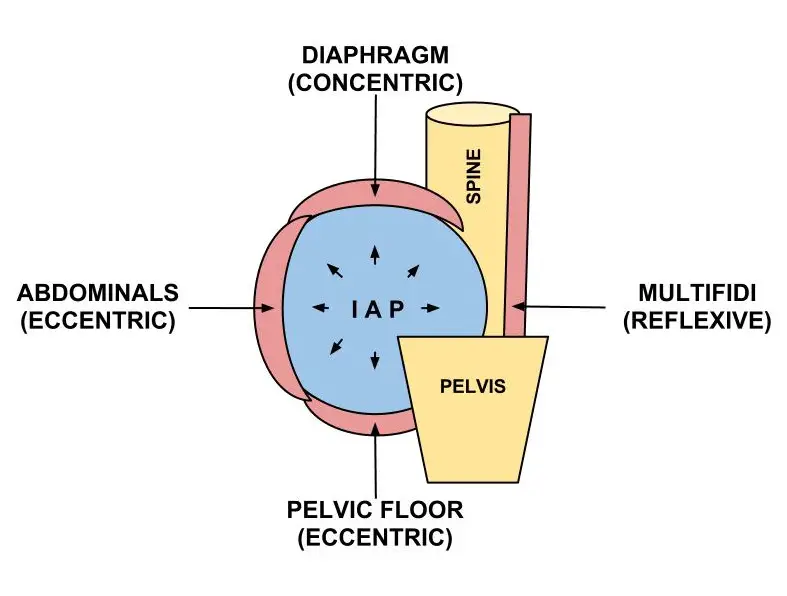
The effect of a proper inhale results in controlled IAP via trunk musculature. The increased IAP anterior to the spine causes a reflexive activation of the posterior spinal stabilizers.
恰當吸氣的效果導致有控制的腹內壓(透過軀幹肌肉)
在脊椎前方升高的腹內壓導致後側的脊椎穩定肌群的反射活化
恰當吸氣的效果導致有控制的腹內壓(透過軀幹肌肉)
在脊椎前方升高的腹內壓導致後側的脊椎穩定肌群的反射活化
Bottom Line 底線
Understanding breathing anatomy and mechanics will allow you to easily assess and intervene respiration. The effects of proper breathing are: adequate respiration, proper biochemical balance, decreased/prevention of psychological distress, and most important for physical therapist – natural activation of the inner core stability.
認識呼吸解剖結構與機制讓我們可以容易的評估與介入呼吸
恰當呼吸的效果是:足夠的呼吸、恰當的生物化學平衡、降低/預防心理痛苦,以及對物理治療師而言最重要的-內核心穩定度的自然活化
Part II will deal with ideal & dysfunctional breathing patterns, assessment, and some simple interventions.
認識呼吸解剖結構與機制讓我們可以容易的評估與介入呼吸
恰當呼吸的效果是:足夠的呼吸、恰當的生物化學平衡、降低/預防心理痛苦,以及對物理治療師而言最重要的-內核心穩定度的自然活化
Part II will deal with ideal & dysfunctional breathing patterns, assessment, and some simple interventions.
Dig Deeper
References
Tom Myers & Leslie Kaminoff. The Breath in the Pelvis – Seminar (NYC 2012).
Courtney R,Reece J (2009). Comparison of the Manual Assessment of Respiratory Motion (MARM) and the Hi Lo breathing assessment determining a simulated breathing pattern. International Journal of Osteopathic Medicine.
Courtney R (2009). The functions of breathing and its dysfunctions and their relationship to breathing therapy. International Journal of Osteopathic Medicine
Courtney R (2011). Dysfunctional Breathing – It’s paramaters, measurement and relevance. Thesis RMIT University. (a must read – click here)
Kaminoff L. (2006). “What yoga therapists should know about the anatomy of breathing.” International Journal of Yoga Therapy.
McLaughlin L. (2009). “Breathing evaluation and retraining in manual therapy.” Journal of Bodywork and Movement Therapies.
McGill S , Sharratt M ,Sequin J P. (1995). “Loads on spinal tissues during simultaneous lifting and ventilatory challenge.” Ergononomics.
Janssens L , Brumagne S, Polspoel K, Toosters T, McConnell A. (2010). “The effect of inspiratory muscles fatigue on postural control in people with and without recurrent low back pain.” Spine.
Hodges P , Heijnen I, Gandevia S C. (2001). “Postural activity of the diaphragm is reduced in humans when respiratory demand increases.” Journal of Physiology.
Hodges P , Butler J ,Mackenzie D K, Gandevia S C. (1997). “Contraction of the human diaphragm during rapid postural adjustments.” Journal of Physiology 505(Pt. 2
Wang S., McGill S (2008). Links Between the Mechanics of Ventilation and Spine Stability. Journal of Applied Biomechanics.
McGill S, Sharratt M & Seguin J (1995). Loads on the spinal tissues during simultaneous lifting and ventilatory challenge. Ergonomics.
Robey J, Boyle K (2009). Bilateral Functional Thoracic Outlet Syndrome in a College Football Player. N Am J Sports Phys Ther.
Boyle K, Olinick J, & Lewis C (2010). The value of blowing up a balloon. N Am J Sports Phys Ther.
Kolar P, Sulc J, Kyncl M, et al. (2010) Stabilizing function of the diaphragm: dynamic MRI and synchronized spirometric assessment. J Appl Physiol.
Kolar P, Sulc J, Kyncl M, et al. (2012). Postural Function of the Diaphragm in Persons With and Without Chronic Low Back Pain. JOSPT.
Hagins M, Lamberg EM (2011). Individuals with low back pain breathe differently than healthy in- dividuals during a lifting task. JOSPT.
Clifton-Stmith T, Rowley J (2011). Breathing pattern disorders and physiotherapy: inspiration for our profession. Physical Therapy Review.
Hruska R (2005). ZOA Position & Mechanical Function. Postural Restoration Institue.
Cook, Gray. Movement: Functional Movement Systems : Screening, Assessment, and Corrective Strategies. Aptos, CA: On Target Publications, 2010.
沒有留言:
張貼留言