
呼吸 Part II -指標/跡象、評估&介入
Part I of this series dealt with breathing anatomy and mechanics. Knowledge and understanding of the anatomy and mechanics of breathing is essential for a proper assessment and intervention. This post will expand on the previous post and go over some indications, assessment, and intervention for breathing.
此系列文章的Part I討論了呼吸解剖構造與機制,對呼吸機制與解剖構造的認識對適當的評估與介入而言是必要的。
本文將會從前文加以細說/擴展並為呼吸介紹一些指標/跡象、評估與介入。
Indications 指標/跡象
So what type of patients do breathing mechanics apply to? Pretty much anyone that moves or breathes.
所以哪種類型的病人是呼吸機制適用的?
幾乎所有會移動或呼吸的人都適用。
幾乎所有會移動或呼吸的人都適用。
Seriously though, you should strongly consider breathing mechanics in all of your patients. Even if it isn’t the main culprit of their dysfunction, it might help return them back to optimal functioning.
說真的,你應該要強烈的為每一位病人考慮到其呼吸機制。
即使呼吸不是他們功能障礙的主要罪魁禍首,也可能能幫助他們回到最佳的功能。
Some more specific examples:
一些更明確的例子:
一些更明確的例子:
- Spine, Hip, and Shoulder Dysfunction
脊椎、髖部與肩部功能障礙 - Postural Faults
姿勢錯誤 - High-Threshold Patterns
高閾值模式 - Impaired Neurodynamics
受損的神經動力學 - Psychological (apprehension, anxiety, central sensitization)
心理的(恐懼、焦慮、中樞敏感化)
Assessment 評估
To keep it simple, you want to visually observe their posture and how they mechanically breathe. Compare this to an ideal breath and look for any signs/symptoms of dysfunctional breathing. Assess this in various postures (supine, seated, standing) and movements. The patient doesn’t need to know. In fact, I find it better if the patient isn’t aware. If you do find a patient with a breathing dysfunction you can then go into a more detailed assessment with palpation techniques (discussed under dysfunctional breathing).
為了保持簡單,我們需要視覺的觀察他們的姿勢與他們機制上是如何呼吸的。
將其與理想呼吸對比並尋找是否有任何功能障礙呼吸的跡象/徵狀
在不同姿勢(仰臥姿、坐姿、站姿)與動作下評估呼吸;病人並不需要知道我們在評估
事實上,我發現如果病人沒有查覺到的話,評估效果更好。
如果你確實發現一個病人有著呼吸功能障礙,就可以接著前進到結合觸診技巧之更為詳細的評估(在功能障礙呼吸底下討論)
Sure, you can make it more complicated by assessing breath holding times, questionnaires, and spirometry. However, this puts the patient through unnecessary discomfort and may affect your rapport. They walked into your clinic because they’re having back pain, not because they want to talk about their breathing patterns and blow into some device.
當然,你也可以透過評估呼吸屏住時間(breath holding times)、問卷與肺量計(spirometry)來讓其變得更複雜。
但是這麼做將會使得病人經歷非必要的不適,且可能會影響到你們的融洽
他們是因為有著背痛才走進你的診所,而不是因為想要討論他們的呼吸模式與吹氣到某些儀器裡面。
It’s important to note that there is a great variance in breathing patterns. Therefore it is difficult to create a protocol and thorough checklist for an ideal breath. However, there is alot of evidence for dysfunctional breathing. So it may be more clinically efficient to look for dysfunctional breathing rather than ideal breathing patterns.
有一點很重要得注意到的是「呼吸模式中有著很大的差異/不同」,因此很難為一個理想呼吸去作出的方案/規程與透徹/絕對的檢查表。
但是目前對於功能障礙的呼吸則有著許多的證據,所以比起尋求理想的呼吸模式來說,去找功能障礙的呼吸可能比較具有臨床效益。
Ideal Breathing 理想的呼吸
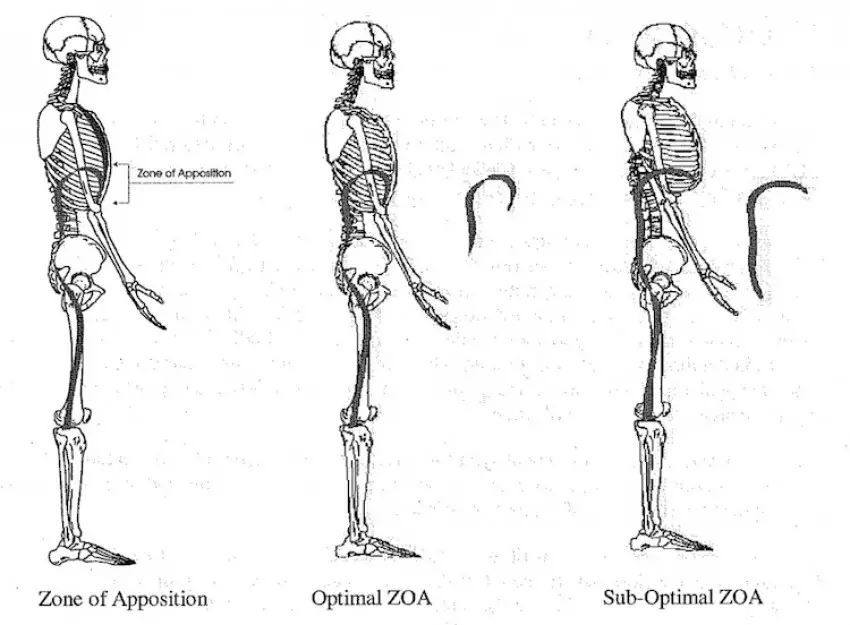
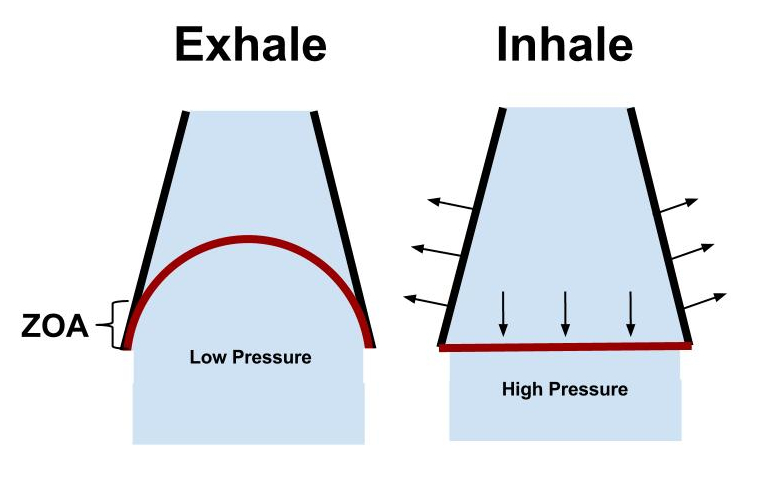
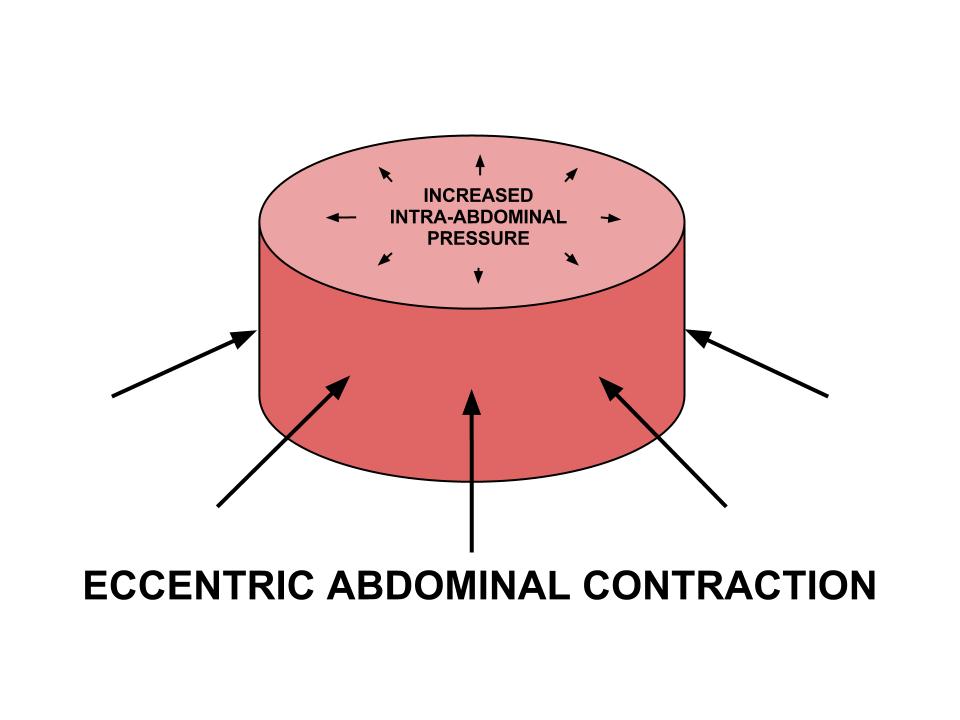
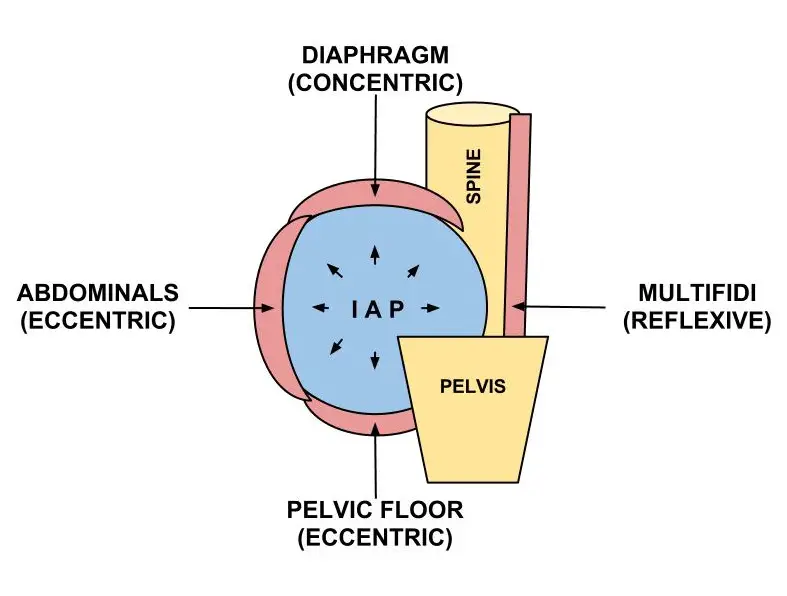
The ideal breath is a smooth, segmental, 3-dimensional motion. During inspiration there is abdominal distension (circumferentially) and a postero-lateral lower ribcage expansion. During expiration there is contraction of abdominals and pelvic floor that returns the ZOA to an optimal position as evident by a depressed sternum and IR of ribs (no anterior ribflare).
理想的呼吸是一個順暢、分段性、3D的動作。
在吸氣過程中會有著腹部的擴張/膨脹(圓周狀)以及下段胸廓的後-側向擴張。
在吐氣過程中會有著將ZOA(並列區域)返回到最佳位置的腹部肌群與骨盆底肌收縮,而這由壓平的胸骨與肋骨的內旋(沒有朝前的肋骨翻/飛起)得以顯見。
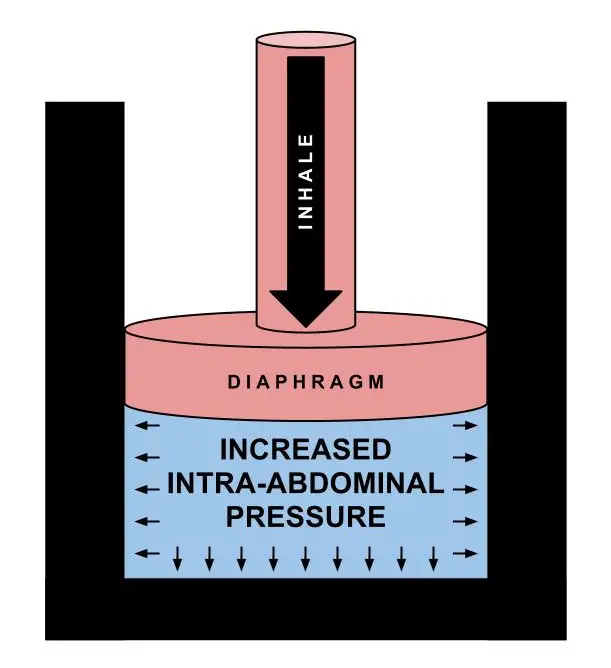
Overall what you’re looking for is the inspiratory cascade of events that leads to controlled increased intra-abdominal pressure and proper muscle activation. On the exhale you want to see adequate expiration of air with no signs of hyperventilation.
總地說來,我們在尋找的是導致有控制之增加的腹內壓與恰當肌肉活化的吸氣級聯事件。
在吐氣時我們希望看到的則是沒有過度換氣跡象之充分的氣體呼出。
Dysfunctional Breathing 功能障礙呼吸
What you never want to see is excessive accessory muscle activation, disproportionate shoulder movement, T-L junction hinging, or vertical ribcage movement. Other signs include: mouth breathing, frequent sighs/throat-clearing, rapid and/or shallow breathes, and asynchronous breaths
我們永遠不會想要看到的是過度的附屬肌肉活化、不成比例的(過大)肩部動作、胸腰椎接合點絞鍊或垂直的胸廓動作;其他的跡象包括:嘴巴呼吸、頻繁的嘆息聲/清嗓、急促與/或短淺的呼吸以及不同步的呼吸。
Paradoxical breathing is a common breathing dysfunction. This is when the patient inhales and there is a vertical and posterior motion of the ribcage and a hollowing of the abdominal cavity.
異位/反常呼吸是一個常見的呼吸功能障礙,此時病人吸氣會有著胸廓的垂直與後向動作以及腹腔的挖空/凹陷
One of the biggest signs of dysfunctional breathing is lack of postero-lateral expansion of the lower ribcage. This can be assessed using the MARM (Manual Assessment of Respiratory Motion).
功能障礙呼吸的其中一個最大跡象就是缺乏下段胸廓的後-側向擴張,而這可以使用MARM(徒手呼吸動作評估)來評估。
Research has shown that the MARM can be be a useful assessment for dysfunctional breathing. This test is simply performed by having the patient seated and facing away from you. You place your fingers on the lower lateral ribcage and align your thumbs with the spine. Then have the patient breath naturally while you assess for the postero-lateral expansion of the lower ribcage. Patrick Ward performs a similar technique in this video around 3:15.
研究已經證明MARM對功能障礙呼吸來說可以是一個很有用的評估,此測試簡單地透過請病人背對我們坐著來執行,我們將手指放置在病人的下段側邊胸廓並將拇指對準病人脊椎,接著請病人自然的呼吸,我們同時評估其下段胸廓的後-側向擴張(Patrick Ward在下列影片的3:15處操作了一個相似的技巧)
High-Threshold Strategy 高閾值策略
This section is purposefully placed between assessment and intervent because it essentially both. A high-threshold strategy is when an individual performs a task using excessive activity/tone in global musculature in a compensatory or protective manner. Gray Cook has described it as when “the body is splinting instead of stabilizing”. One of the major signs of this strategy is dysfunctional breathing patterns.
此區塊有目的的被擺在評估與介入中間,因為其對兩者都是不可少的
高閾值策略是人們以一個代償性或保護性方式在整體肌肉使用過度活動/張力來執行任務之時。
Gray Cook將其描述為"身體正在夾板固定而非穩定的時候",此種策略其中一個最主要的跡象就是功能障礙的呼吸模式。
An example of this is when you give a patient an exercise that is too difficult for them. They start to hold their breath and squeeze every muscle they have. A patient won’t be able to perform a proper breathing pattern if they are using a high-threshold strategy.
關於此種策略的一個例子就是當我們給病人一個對他們而言太困難的運動時,他們開始閉住呼吸然後繃緊他們有的所有肌肉,「如果他們正使用著高閾值策略,是無法執行恰當的呼吸模式的」。
So how do you use this to your advantage? You can use breathing assessment throughout all of your interventions to verify that the patient is not using a high-threshold strategy to perform the task.
所以我們要如何好好使用這種優勢?
我們可以在所有我們的介入中使用呼吸評估來驗證/檢驗病人並沒有使用高閾值策略來執行任務。
Intervention 介入
There are many ways to treat breathing dysfunctions. Which rabbit hole you go down depends on your patient and what they need.
有許多的方式可以治療呼吸功能障礙,我們要跳進哪個兔子坑取決於病人所需。
However, the first place to start for everyone should be from an educational stand-point. It is advantageous to explain to the patient why breathing is important to them specifically (use knowledge from Part I).
然而,對每個人來說的第一個出發點都應該要從一個教育性的觀點開始,對病人解釋為何呼吸對他們那麼的重要是有利的。(使用Part I的知識)
Then you should teach the patient about dysfunctional breathing and what you expect for a proper breath. To avoid overcomplicating this, I usually simply give the patient a cue that has them focus on the circumferential lower ribcage and abdominal distension.
然後我們應該要教導病人什麼是功能障礙的呼吸以及你所期待的恰當呼吸,為了避免將此過度複雜化,我通常會單純地給病人一個要他們專注在還狀面/圓頂狀的下段胸廓與腹部膨脹的提示。
Some example cues I’ve heard and used: “breath into your lower ribs and abs”, “breath into an imaginary belt around your stomach”, “breath down and out”, “inhale into a balloon inside your stomach”, “push your breath down”, “expand your ribs out with your breath” etc. The possibilities are endless.
有些我曾聽過與使用的範例提示:「吸氣進入你的下段肋骨與腹部」、「吸氣進入一個環繞於胃部的想像腰帶」、「向下向外吸氣」、「將氣吸入一個在胃部裡面的氣球」、「將你的吸氣向下推」、「透過你的呼吸擴張肋骨」之類的
可能性是無窮盡的
You can also use tactile cues. Put your hands or a theraband around their lower ribcage to increase sensory afferent input. Then have them to breath into the resistance of your hands/theraband.
你也可以使用觸覺提示,將雙手或環圈彈力帶放置在病人的下段胸廓來增加感覺輸入,接著請他們吸氣進入我們雙手/環圈彈力帶的阻力。
For patients who have great difficulty with this or use paradoxical breathing patterns you may need to start simple. I usually start with a simple progression of hi-lo breathing, lateral expansion breathing, and finally a combination of the two for an “ideal breath”.
對使用此種方式遭遇相當困難或使用異位呼吸模式的病人來說,我們或許應該要再簡單一點來開始。
我通常由簡單的Hi-Lo呼吸進程、側向擴張的呼吸來開始,最終將兩者結合在一起操作來達成"理想呼吸"。
It’s important to educate them and have them feel the difference in their hands and their body. As the patient gets comfortable you can cue the patient to breath in through the nose and out through the mouth, exhale longer than the inhale, and try to expire all of their air.
教育病人並讓他們感覺雙手之間的差異和自身身體是很重要的,當病人變得自在舒服,我們就可以提示病人透過鼻子吸氣、透過嘴巴吐氣、吐氣要長於吸氣,並試著呼出體內所有的空氣。
Other biomechanical interventions can be separated into mobility and stability categories. Part I focused on the stability aspect of the inspiration, but it can also be used for mobility (yoga has been doing this for thousands of years).
其他的生物力學介入可以被分成活動度與穩定度的類別,Part I聚焦在吸氣的穩定度面,但其也可以被用於活動度的改善(瑜珈已經這麼做上千年了)。
Mobility 活動度
Much like ligament locking for joint mobilization/manipulation, the breath can be directed by altering postures and positions. Leslie Kaminoff describes breathing as the act of “shape changing”. Using this theory you can alter your posture to direct the where the breath (“shape change”) occurs. It’s physics. The shape change from inspiration (expansion) will always go towards the place of least resistance.
很像是關節鬆動術的ligament locking,呼吸可以透過改變姿勢與位置來被導向。
Leslie Kaminoff將呼吸描述為一個"型態變化"的行為,運用這個理論我們可以改變姿勢來引導呼吸(型態變化)發生的位置/地方,這是物理現象。
來自吸氣(擴張)的型態變化總會朝最少阻力的地方前進。
For example, if a patient has a restricted R posterior lumber quadrant, then you would put them in a childs pose reaching contralaterally with their R UE. Since you closed off the L side by laterally sidebending/flexing and closed off the anterior R rib cage by flexing, the only place for the shape change to occur would be into the R posterior quadrant.
舉例來說,如果一個病人有著受限的右方後側腰部象限,我們會請他呈現嬰兒姿、並以他的右上肢向其對側延伸。
因為我們透過側向的側彎/屈曲將左側封鎖起來以及透過屈曲將前側的右胸廓封鎖起來,為一個能夠有型態變化發生進入的地方就是右方後側的象限。
You can further increase the expansion (stretch) into this area using tactile or verbal cues to get them to breath into the postero-lateral R rib cage.
我們可以使用觸覺或口語提示讓病人呼吸進入後-側邊的右胸廓以更進一步的將擴張增加進入此區域。
Another mobility aspect of breathing is it’s amplification of the parasympathetic NS. This can be very advantageous when performing manual techniques or corrective exercises to increase tissue extensibility. Muscle guarding and reflexive activation can be minimized by focusing on breathing.
呼吸活動度的其他面向是其對副交感神經系統的放大/增幅,在在執行徒手技巧或矯正性運動以增加組織延展性時會非常的有利
透過專注在呼吸,肌肉防衛與反射性活化可以被最小化
Stability 穩定度
As mentioned before with the high-threshold strategies, simply having your patient breath properly during exercises will help establish proper inner core stabilization.
如前面所提到的高閾值策略,單純讓病人在運動過程中恰當的呼吸將能幫助建立恰當的內部核心穩定性。
One important consideration is that you must simultaneously monitor their posture. You always want a neutral spine. Performing a task with an anterior pelvic tilt not only causes compensatory mechanisms, but it prevents proper breathing mechanics (decreased ZOA, decreased eccentric abdominal & PF contraction).
有個重要的考慮事項就是你必須要同時監控他們的姿勢,要他們保持中立的脊椎
帶著前傾的骨盆執行任務不只會造成代償性的機制,也會無法有著恰當的呼吸機制(減小的ZOA、減小的離心腹部肌群&骨盆底肌收縮)
Again, the guy with a positive scour sign, hip impingement, and anterior pelvic tilt doesn’t want to hear about breathing. He just wants his hip to stop hurting so he can get back to golfing. So instead of going into too much detail about the mechanics of breathing or working on isolated breathing exercises, simply have your patient breath with a neutral spine during all their exercises. It’s a great place to start and ensures that the patient is performing the exercise with the correct musculature.
再一次,有著陽性腹瀉跡象、髖部夾擠與骨盆前傾的傢伙不會想要聽關於呼吸的事,他只想要髖部不再痛讓他可以回去繼續打高爾夫球。
所以與其給太多關於呼吸機制的細節(或研究得太細)或致力再孤立的呼吸運動上,不如單純請病人在其所有的運動中以一個中立脊椎呼吸
這是一個確保病人以正確肌肉執行運動與開始的好地方。
Since I have learned about the importance of breathing I no longer time my patients with a stopwatch. I now have everyone counting their breaths (i.e. holding quadruped diagonals for 7 breathes instead of 30 sec).
因為我已經學到關於呼吸的重要性,我不再使用碼表來為我的病人計時,現在我都請每位病人數他們的呼吸(維持在四足跪姿斜向延伸的動作行7個呼吸來取代30秒)
For advanced patients you can progress to “breathing behind the shield”. This is a term coined by the great Pavel Tsatouline. It’s a great way to incorporate breathing with core stability. It describes the act of maintaining abdominal tension while breathing.
對進階的病人我們可以進階到"在盾牌後方呼吸"
這是一個由Pavel Tsatouline所創造的詞,它描述的是在呼吸時維持腹部張力的行為。
“Breathing behind the shield” is the balance of controlling intra-abdominal pressure and abdominal & pelvic floor muscle tone. It displays that the patient is able to use the diaphragm’s dual function: respiration and stabilization.
"在盾牌後方呼吸"是控制腹內壓與腹部&骨盆底肌肌肉張力的平衡,它顯示出該病人可以使用橫膈膜的雙重功能:呼吸與穩定性
Hans Lindgren has an amazing video on assessing and interventions for breathing and core stability. At about 2:10 into the video he goes over a great technique to help you teach your patients how to “breath behind the shield”. This is a great place to begin and can be progressed through the developmental sequence.
大約在影片中的2:10處他探討了一些幫助我們教導病人如何"在盾牌後方呼吸"的超棒技巧,而這正是一個好的開始點,且可以透過發展順序來被進程/進階。
Bottom Line 底線
There are many ways to assess and treat dysfunctional breathing patterns. Hopefully this article will give you a good place to start. Below are some great articles, videos, and descriptions of breathing patterns. As with every intervention, it is important to master this yourself before you try to teach your patient.
評估與治療功能障礙呼吸模式的方法很多,希望本文能給讀者們一個好的開始點下方是一些關於呼吸模式的好文、好影片與描述
和所有的介入一樣,在試著教給病人之前自己先熟練/精通是非常重要的。
Dig Deeper
Simple Exercise – Crocodile Breathing
References
Tom Myers & Leslie Kaminoff. The Breath in the Pelvis – Seminar (NYC 2012).
Courtney R,Reece J (2009). Comparison of the Manual Assessment of Respiratory Motion (MARM) and the Hi Lo breathing assessment determining a simulated breathing pattern. International Journal of Osteopathic Medicine.
Courtney R (2009). The functions of breathing and its dysfunctions and their relationship to breathing therapy. International Journal of Osteopathic Medicine
Courtney R (2011). Dysfunctional Breathing – It’s paramaters, measurement and relevance. Thesis RMIT University. (a must read – click here)
Kaminoff L. (2006). “What yoga therapists should know about the anatomy of breathing.” International Journal of Yoga Therapy.
McLaughlin L. (2009). “Breathing evaluation and retraining in manual therapy.” Journal of Bodywork and Movement Therapies.
McGill S , Sharratt M ,Sequin J P. (1995). “Loads on spinal tissues during simultaneous lifting and ventilatory challenge.” Ergononomics.
Janssens L , Brumagne S, Polspoel K, Toosters T, McConnell A. (2010). “The effect of inspiratory muscles fatigue on postural control in people with and without recurrent low back pain.” Spine.
Hodges P , Heijnen I, Gandevia S C. (2001). “Postural activity of the diaphragm is reduced in humans when respiratory demand increases.” Journal of Physiology.
Hodges P , Butler J ,Mackenzie D K, Gandevia S C. (1997). “Contraction of the human diaphragm during rapid postural adjustments.” Journal of Physiology 505(Pt. 2
Wang S., McGill S (2008). Links Between the Mechanics of Ventilation and Spine Stability. Journal of Applied Biomechanics.
McGill S, Sharratt M & Seguin J (1995). Loads on the spinal tissues during simultaneous lifting and ventilatory challenge. Ergonomics.
Robey J, Boyle K (2009). Bilateral Functional Thoracic Outlet Syndrome in a College Football Player. N Am J Sports Phys Ther.
Boyle K, Olinick J, & Lewis C (2010). The value of blowing up a balloon. N Am J Sports Phys Ther.
Kolar P, Sulc J, Kyncl M, et al. (2010) Stabilizing function of the diaphragm: dynamic MRI and synchronized spirometric assessment. J Appl Physiol.
Kolar P, Sulc J, Kyncl M, et al. (2012). Postural Function of the Diaphragm in Persons With and Without Chronic Low Back Pain. JOSPT.
Hagins M, Lamberg EM (2011). Individuals with low back pain breathe differently than healthy in- dividuals during a lifting task. JOSPT.
Clifton-Stmith T, Rowley J (2011). Breathing pattern disorders and physiotherapy: inspiration for our profession. Physical Therapy Review.
Hruska R (2005). ZOA Position & Mechanical Function. Postural Restoration Institue.
Cook, Gray. Movement: Functional Movement Systems : Screening, Assessment, and Corrective Strategies. Aptos, CA: On Target Publications, 2010.
—
The main reason I do this blog is to share knowledge and to help people become better clinicians/coaches. I want our profession to grow and for our patients to have better outcomes. Regardless of your specific title (PT, Chiro, Trainer, Coach, etc.), we all have the same goal of trying to empower people to fix their problems through movement. I hope the content of this website helps you in doing so.
If you enjoyed it and found it helpful, please share it with your peers. And if you are feeling generous, please make a donation to help me run this website. Any amount you can afford is greatly appreciated.
{kind=link}